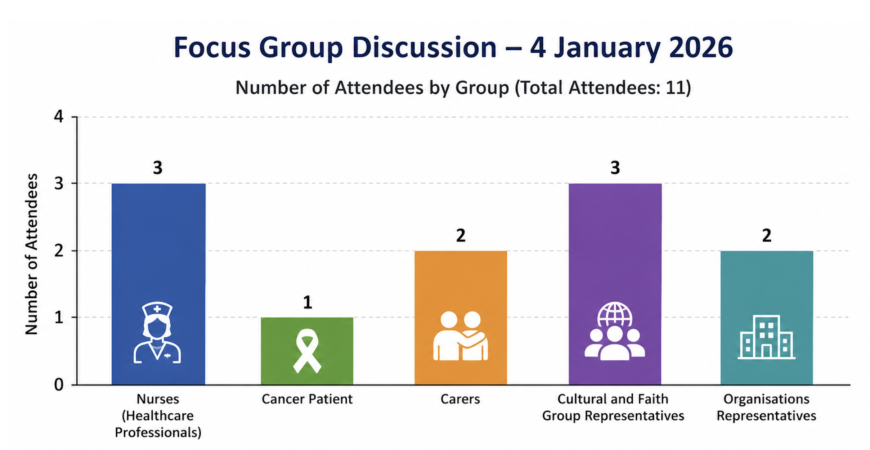
On 4 January 2026, the Punya Foundation convened a face-to-face community consultation to address disparities in cancer awareness, screening, and oncology support within Nepali-speaking communities in Australia. Coordinated by Dr. Lakshmi Prasad Dhakal, the session integrated insights from 11 key stakeholders, including three registered nurses, one cancer patient, two primary carers, three faith leaders, and two community executives.
Core findings and barriers
1. Socio-cultural stigma and diagnostic fear
Cancer remains a highly sensitive topic within many Nepali language speaking families. Deeply rooted cultural misconceptions and a fatalistic view of the disease create a climate of fear, discouraging open dialogue about symptoms and diagnoses. Because families fear social isolation, individuals often delay seeking medical advice. This culture of silence directly leads to late-stage presentations, making the activation of trusted community anchors, such as faith leaders and survivors, essential to reframing cancer as a treatable illness.
2. Underutilisation of free screening programs
A substantial knowledge gap persists regarding Australia’s preventative medicine framework. A significant portion of the community is unaware that vital diagnostic pipelines, such as BreastScreen and national cervical and bowel screening programs, are publicly funded and free. Mainstream, digital-only public health campaigns fail to reach this demographic, highlighting the need for grassroots, in-person information sessions delivered in culturally safe environments.
3. Linguistic and systemic isolation
Navigating general practitioner referrals, Medicare billing, and complex medical jargon poses a severe challenge for older demographics and newly arrived migrants. While federal translating services are available, a unique interpreter paradox exists. Many individuals decline these services due to acute privacy concerns within a small, interconnected migrant community, leading to heightened patient anxiety and delayed clinical decision-making.
4. Practical and structural obstacles
- Socio-economic pressures: Rigid work schedules and casual employment force community members to prioritise immediate income over preventative health appointments.
- Logistical friction: Public transport dependencies and geographic distance from major metropolitan tertiary hospitals create physical barriers to attending consecutive oncology treatments.
- Support isolation: Many families remain completely unaware of existing psychosocial resources, such as subsidised patient transport schemes, Cancer Council helplines, or carer respite benefits.
Strategic recommendations
To bridge these gaps, stakeholders recommended a coordinated intervention strategy focused on three pillars:
- Bilingual education: Deliver a year-round schedule of localised health literacy workshops in native languages to normalise preventative checks.
- Community advocacy: Train cultural leaders and survivors as “Multicultural Health Champions” to build trust between public health providers and insular networks.
- System integration: Establish formal partnerships between multicultural organisations and local health networks to streamline patient referral pathways.
- Create peer-groups to share lived experience and to empower talking about cancer.